CML Treatment Options: Tyrosine Kinase Inhibitors for Chronic Myeloid Leukemia
Chronic Myeloid Leukemia (CML) is a type of blood cancer that begins in the bone marrow and affects the production of white blood cells. It is primarily caused by a genetic abnormality known as the Philadelphia chromosome, which creates the BCR-ABL1 fusion gene. This abnormal gene produces an abnormal tyrosine kinase protein that drives uncontrolled leukemia cell growth.
The introduction of Tyrosine Kinase Inhibitors (TKIs) has transformed CML treatment, turning what was once a life-threatening disease into a manageable long-term condition for many patients. Modern treatment focuses on targeted therapy, molecular monitoring, and personalized medicine based on mutation profile and treatment response.
This guide explains first-line and second-line CML treatment options, compares major TKIs such as Imatinib, Dasatinib, Nilotinib, Bosutinib, Ponatinib, and Asciminib, and highlights safe medicine access for patients requiring prescription cancer therapy.
What Is Chronic Myeloid Leukemia (CML)?
CML progresses through three phases: chronic phase (most common at diagnosis), accelerated phase, and blast phase (resembling acute leukemia). In the chronic phase, many patients have mild or no symptoms, and the disease can often be managed effectively with oral medications for years.
The hallmark of CML is the BCR-ABL fusion gene, which produces a tyrosine kinase protein that drives uncontrolled white blood cell production. Modern treatments target this pathway directly, transforming CML from a life-threatening condition into a manageable chronic illness for the majority of patients in the chronic phase.
First-Line Treatment for Chronic Phase CML
For most newly diagnosed patients with chronic-phase CML, treatment begins with a first-line Tyrosine Kinase Inhibitor. These medicines block the BCR-ABL tyrosine kinase enzyme, stopping leukemia cell growth at the molecular level.
First-line therapy aims to achieve:
- Complete Hematologic Response (CHR)
- Complete Cytogenetic Response (CCyR)
- Major Molecular Response (MMR)
- Deep Molecular Response (DMR)
The most commonly used first-line TKIs include:
- Imatinib
- Dasatinib
- Nilotinib
- Bosutinib (selected cases)

Choice depends on:
- patient age
- cardiovascular risk
- liver function
- lung disease history
- mutation analysis
- pregnancy planning
- treatment affordability
Early response monitoring through BCR-ABL PCR testing is essential for evaluating treatment success.
Second-Line and Resistant CML Therapy
If first-line therapy fails due to resistance, intolerance, or inadequate molecular response, second-line treatment becomes necessary.
Treatment decisions are guided by:
- BCR-ABL mutation testing
- ELN response milestones
- adverse event profile
- disease progression risk
Second-line options include:
- Bosutinib
- Ponatinib
- Asciminib
- stem cell transplantation (selected advanced cases)
Resistance may occur because of kinase domain mutations, poor adherence, or disease progression to accelerated or blast phase.
Main CML Treatment Options: Tyrosine Kinase Inhibitors (TKIs)
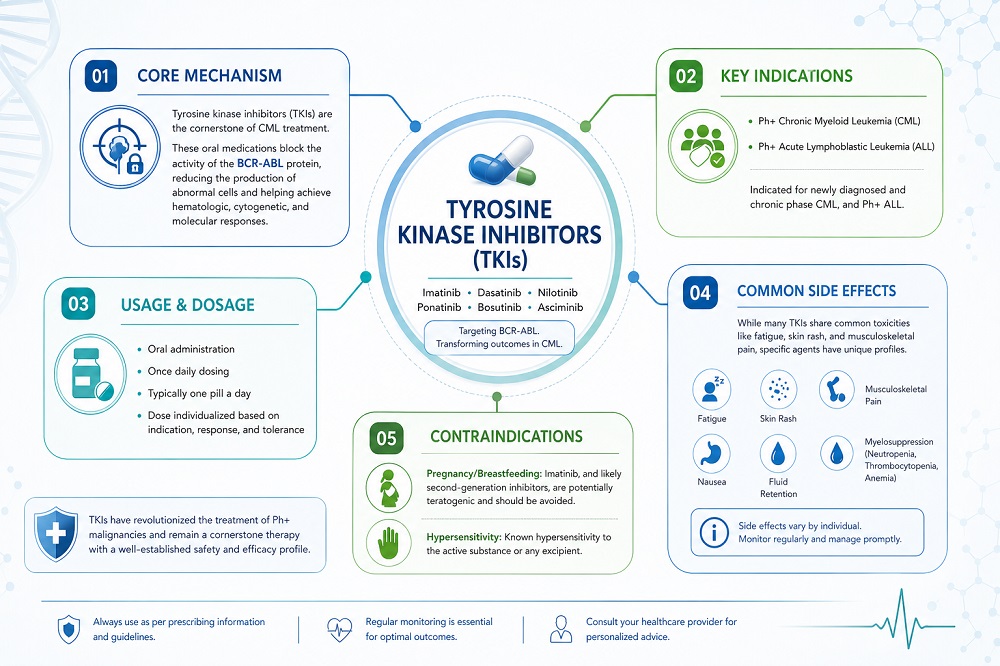
Tyrosine kinase inhibitors (TKIs) are the cornerstone of CML treatment. These oral medications block the activity of the BCR-ABL protein, reducing the production of abnormal cells and helping achieve hematologic, cytogenetic, and molecular responses.
Commonly used TKIs include:
- Imatinib (Gleevec or generic versions) – First-generation TKI, often used as a first-line option due to its long track record and tolerability profile.
- Dasatinib (Sprycel) – Second-generation TKI, potent against many BCR-ABL mutations.
- Nilotinib (Tasigna) – Second-generation TKI, taken twice daily.
- Bosutinib (Bosulif) – Second-generation TKI with a distinct side effect profile.
- Ponatinib (Iclusig) – Third-generation TKI, often reserved for patients with the T315I mutation or after failure of other TKIs.
- Asciminib (Scemblix) – A newer allosteric inhibitor that binds to a different site on the BCR-ABL protein, offering an option for patients with resistance or specific needs.
Selection of the initial TKI depends on factors such as Sokal or ELTS risk score, patient age, comorbidities (e.g., cardiovascular disease, lung issues, or gastrointestinal conditions), potential drug interactions, and lifestyle considerations. Generic versions of imatinib and dasatinib are available in many markets, which can influence accessibility.

Treatment Phases and Strategies
Chronic Phase CML
Most patients are diagnosed in the chronic phase. The goal is to achieve and maintain a deep molecular response (major molecular response or better) while minimizing side effects. Treatment usually starts with a TKI as monotherapy. Regular monitoring with complete blood counts and quantitative PCR for BCR-ABL transcript levels guides ongoing management.
In some patients who achieve sustained deep molecular responses (typically after several years of therapy), treatment-free remission (TFR) may be considered under close specialist supervision with frequent molecular monitoring. Not all patients are eligible, and restarting therapy promptly is required if molecular response is lost.
Advanced Phase CML (Accelerated or Blast Phase)
For accelerated or blast phase disease, treatment is more intensive. Options may include a more potent TKI (possibly combined with chemotherapy), clinical trials, or preparation for allogeneic stem cell transplantation in eligible patients. Outcomes are generally less favorable than in chronic phase, highlighting the importance of early diagnosis and effective frontline therapy.
Other CML Treatment Approaches
While TKIs are the primary treatment, additional options may be considered in specific situations:
- Interferon-alpha: Rarely used today but may have a role in select cases, sometimes in combination.
- Chemotherapy: Used in blast phase or in combination with TKIs for advanced disease.
- Allogeneic stem cell transplant: Potentially curative for younger, fit patients with high-risk disease, TKI resistance, or advanced phase CML. It carries significant risks and is reserved for appropriate candidates.
- Clinical trials: Ongoing research explores new TKIs, combinations, and strategies to improve depth of response or enable safer treatment discontinuation.
Supportive care, including medications for side effect management, infection prevention, and addressing comorbidities, plays a vital role throughout treatment.
Safety Considerations and Side Effects of CML Treatments
TKIs are generally well-tolerated compared to traditional chemotherapy, but they can cause side effects that vary by drug. Common issues include fatigue, gastrointestinal symptoms (diarrhea, nausea), rash, muscle or joint pain, and fluid retention. Specific concerns include:
- Cardiovascular risks with some second-generation TKIs.
- Pulmonary effects or pleural effusion with dasatinib.
- Liver enzyme elevations or QT prolongation with certain agents.
- Pancreatic or vascular issues with others.
Regular monitoring of blood counts, liver and kidney function, heart health, and molecular response is essential. Many side effects can be managed with dose adjustments, temporary interruptions, supportive medications, or switching to a different TKI. Patients should report new symptoms promptly to their care team.
Important: Individual tolerability differs. Pregnancy is contraindicated with most TKIs due to potential fetal harm; effective contraception and family planning discussions with specialists are recommended.
Factors Influencing CML Treatment Choices
Oncologists tailor therapy based on:
- Disease risk score at diagnosis.
- Patient’s overall health and comorbidities.
- Potential drug interactions and lifestyle factors (e.g., dosing schedule).
- Cost and insurance coverage (generics vs. branded medications).
- Goals of care, including desire for future treatment-free remission.
Shared decision-making between patient and physician is key. Second opinions from CML specialists can provide additional perspectives, especially in complex or resistant cases.
FAQs About CML Treatment Options
What are the main CML treatment options?
The primary treatments for chronic myeloid leukemia are tyrosine kinase inhibitors (TKIs) such as imatinib, dasatinib, nilotinib, bosutinib, ponatinib, and asciminib. These targeted oral medications form the foundation of therapy in the chronic phase. In advanced phases, combinations with chemotherapy or stem cell transplant may be considered.
Which TKI is best for newly diagnosed CML?
No single TKI is universally best. Choice depends on risk score, patient comorbidities, side effect profiles, and other factors. Imatinib is often suitable for many patients, while second-generation TKIs may be preferred in higher-risk cases. Your doctor will recommend the most appropriate option.
Can CML treatment be stopped?
In select patients who achieve and maintain a deep molecular response for a sufficient duration, treatment-free remission (TFR) may be attempted under close monitoring. Not everyone qualifies, and regular PCR testing is required. Restarting therapy is usually effective if response is lost.
How long do patients take TKIs for CML?
Many patients continue TKI therapy long-term or indefinitely. Duration depends on response depth, tolerability, and whether treatment-free remission is pursued. Regular molecular monitoring guides decisions.
What are common side effects of CML TKIs?
Side effects vary by drug but may include fatigue, diarrhea, rash, muscle pain, fluid retention, or laboratory abnormalities. Specific risks (e.g., cardiovascular or pulmonary) differ between agents. Most can be managed with supportive care or dose changes.
Is there a cure for CML?
TKIs do not typically cure CML but can provide excellent long-term control. Allogeneic stem cell transplant offers a potential cure for some patients but carries significant risks and is usually reserved for advanced or resistant disease.
Are generic TKIs available for CML?
Yes. Generic versions of imatinib and dasatinib are widely available and can improve affordability while maintaining therapeutic equivalence to brand-name products.
What happens if CML becomes resistant to a TKI?
Resistance can occur due to mutations or other mechanisms. Options include switching to a different TKI (e.g., ponatinib for T315I mutation), dose escalation, combination approaches, or clinical trials. Mutation testing helps guide next steps.
Can lifestyle changes support CML treatment?
While not a substitute for medication, maintaining a healthy diet, regular exercise (as approved by your doctor), stress management, and medication adherence support overall well-being during treatment.
Is stem cell transplant a common CML treatment?
No, it is not first-line for most chronic-phase patients. It may be considered for younger patients with high-risk features, TKI intolerance/resistance, or advanced-phase disease.
How is response to CML treatment monitored?
Monitoring includes regular blood tests for complete blood counts and quantitative PCR to measure BCR-ABL transcript levels. Bone marrow assessments may be needed initially or if response is suboptimal.
Are new CML treatments in development?
Research continues into novel TKIs, combinations, and strategies to deepen responses or improve treatment-free remission rates. Clinical trials offer access to emerging options for eligible patients.
Conclusion
CML treatment options have advanced significantly with the development of multiple generations of tyrosine kinase inhibitors. For most patients in the chronic phase, oral TKIs provide effective disease control, allowing many to live active lives with careful monitoring. Treatment selection is personalized, balancing efficacy, safety, and individual circumstances.
While excellent outcomes are achievable, ongoing follow-up with a hematology specialist experienced in CML is crucial for optimizing therapy, managing side effects, and exploring options like treatment-free remission when appropriate.
If you or a loved one has been diagnosed with CML, discuss all available options, monitoring plans, and support resources with your healthcare team. Leukemia support organizations and CML-specific patient groups can offer additional education and community support.
Disclaimer: This article is educational and based on general information about CML treatment approaches. It does not replace professional medical advice, diagnosis, or treatment. Treatment guidelines evolve, and individual recommendations vary. Always consult your physician for personalized care.
