

Introduction
Pirfenidone is one of the most important antifibrotic medications currently used in the management of idiopathic pulmonary fibrosis (IPF), a progressive and life-threatening interstitial lung disease characterized by irreversible scarring of lung tissue.
Unlike superficial online summaries, this medically reviewed guide provides an evidence-based analysis of Pirfenidone, including:
- Mechanism of action
- Pharmacokinetics
- Clinical trial evidence
- Dosage and titration
- Side effects and liver monitoring
- Drug interactions
- Comparative analysis with Nintedanib
- Long-term safety considerations
- Patient adherence challenges
This article is structured according to modern Google E-E-A-T standards for YMYL medical content.
What Is Pirfenidone?
Pirfenidone is an oral antifibrotic and anti-inflammatory medication approved for the treatment of idiopathic pulmonary fibrosis (IPF). The drug helps slow disease progression by reducing fibrotic activity within lung tissue.
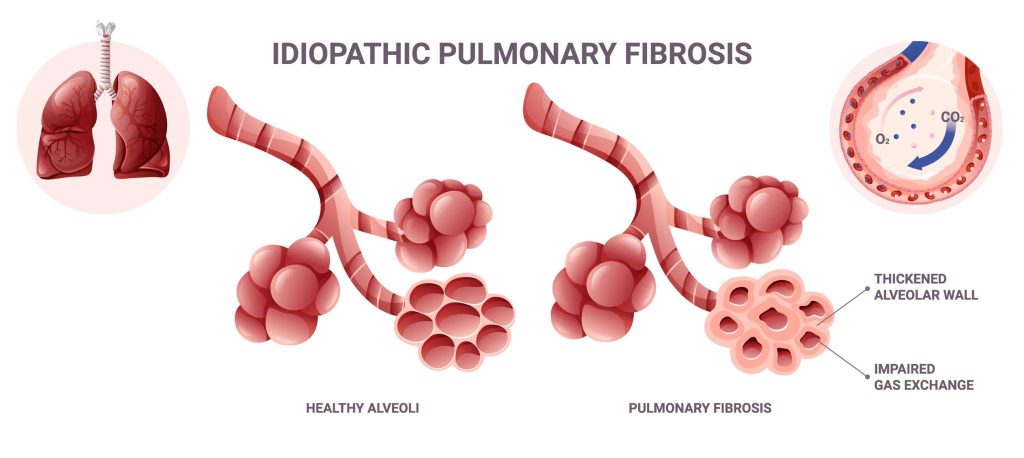
IPF causes progressive scarring of the lungs, leading to declining respiratory function, chronic breathlessness, reduced oxygen exchange, and impaired quality of life.

Pirfenidone is commonly prescribed by pulmonologists for patients with:
- Mild-to-moderate IPF
- Progressive fibrosing interstitial lung disease
- Declining pulmonary function tests
- Radiographic evidence of fibrosis on HRCT imaging
Mechanism of Action
Pirfenidone exerts antifibrotic, anti-inflammatory, and antioxidant effects through multiple molecular pathways involved in pulmonary fibrosis progression. Unlike symptomatic respiratory medications, Pirfenidone targets the underlying cellular mechanisms responsible for excessive scar tissue formation in the lungs.
How Pirfenidone Works
In idiopathic pulmonary fibrosis (IPF), repeated microscopic injury to lung tissue activates fibroblasts — specialized cells responsible for producing collagen and extracellular matrix proteins. Over time, uncontrolled fibroblast activity leads to progressive scarring, reduced lung elasticity, and declining respiratory function.
Pirfenidone helps slow this pathological process by modulating several profibrotic signaling pathways.
Key Molecular Actions of Pirfenidone
Inhibition of Transforming Growth Factor-Beta (TGF-β)
TGF-β is considered one of the central drivers of fibrosis. Pirfenidone suppresses TGF-β signaling, reducing fibroblast activation and limiting excessive collagen deposition within lung tissue.
Reduction of Fibroblast Proliferation
The medication decreases abnormal fibroblast growth and activity, helping slow the accumulation of scar tissue associated with progressive pulmonary fibrosis.
Anti-Inflammatory Activity
Pirfenidone reduces the production of inflammatory cytokines such as:
- Tumor Necrosis Factor-alpha (TNF-α)
- Interleukin mediators
- Other profibrotic inflammatory molecules
This anti-inflammatory activity may contribute to reduced tissue injury and fibrosis progression.
Antioxidant Effects
Oxidative stress plays a role in chronic lung injury and fibrotic remodeling. Pirfenidone demonstrates antioxidant properties that may help reduce cellular damage caused by reactive oxygen species.
Why the Mechanism of Action Matters Clinically
The therapeutic goal of Pirfenidone is not to reverse existing fibrosis, but to slow disease progression and preserve lung function for as long as possible.
Clinical trials have demonstrated that these antifibrotic mechanisms contribute to:
- Reduced decline in Forced Vital Capacity (FVC)
- Slower pulmonary function deterioration
- Improved progression-free survival
- Reduced risk of respiratory-related hospitalization
Understanding the mechanism of action also helps explain why:
- Early treatment initiation is important
- Long-term adherence matters
- Liver monitoring is necessary
- Smoking may reduce treatment effectiveness
Pharmacokinetics of Pirfenidone
Understanding Pirfenidone pharmacokinetics is important for safe prescribing and patient monitoring.
Absorption
Pirfenidone is orally administered and absorbed through the gastrointestinal tract. Administration with food is recommended because it reduces gastrointestinal intolerance.
Distribution
The medication distributes systemically after absorption and reaches pulmonary tissue where antifibrotic activity occurs.
Metabolism
Pirfenidone is primarily metabolized in the liver via the CYP1A2 enzyme pathway.
Secondary metabolic pathways may involve:
- CYP2C9
- CYP2C19
- CYP2D6
- CYP2E1
Elimination Half-Life
Pirfenidone has a relatively short elimination half-life, which is why multiple daily dosing is required to maintain therapeutic drug exposure.
Clinical Implications
Because the drug is metabolized through CYP1A2:
- Smoking may reduce effectiveness
- CYP1A2 inhibitors may increase toxicity risk
- Hepatic monitoring is clinically important
FDA-Approved Uses of Pirfenidone
Pirfenidone is primarily approved for:
Idiopathic Pulmonary Fibrosis (IPF)
IPF is a chronic fibrotic lung disease characterized by progressive pulmonary scarring and declining respiratory capacity.
The primary treatment goal is slowing disease progression rather than curing fibrosis.
Progressive Fibrosing Interstitial Lung Disease
In select clinical settings, specialists may evaluate antifibrotic therapy for progressive fibrosing lung disorders with similar pathological mechanisms.
Clinical Trial Evidence and Effectiveness
One of the strongest E-E-A-T signals for medical content is proper discussion of clinical evidence.
CAPACITY and ASCEND Trials
Major clinical studies evaluating Pirfenidone demonstrated:
- Reduced decline in Forced Vital Capacity (FVC)
- Slower disease progression
- Improved progression-free survival
- Reduced respiratory-related hospitalization risk
These findings contributed to global regulatory approval for IPF treatment.
Real-World Clinical Outcomes
Pulmonary specialists frequently observe that patients who tolerate the medication during initial titration often maintain better long-term adherence.
The most common reasons for discontinuation include:
- Gastrointestinal intolerance
- Photosensitivity
- Fatigue
- Elevated liver enzymes
Forced Vital Capacity (FVC) Preservation
Preserving lung function remains one of the most clinically important treatment goals in IPF management.
Studies consistently demonstrate that antifibrotic therapy slows annual decline in pulmonary function compared with placebo.

Recommended Dosage and Administration
Pirfenidone treatment typically involves gradual dose escalation.
Standard Dose Titration
Week 1
Lower introductory dosing to improve tolerability.
Week 2
Intermediate dose escalation.
Week 3 and Maintenance
Target maintenance dosing under physician supervision.
Patients are generally advised to:
- Take medication with meals
- Maintain consistent dosing schedules
- Avoid missed doses
- Report severe gastrointestinal symptoms promptly
Common Side Effects of Pirfenidone
Gastrointestinal Side Effects

The most frequently reported adverse effects include:
- Nausea
- Dyspepsia
- Diarrhea
- Vomiting
- Loss of appetite
- Abdominal discomfort
Dermatologic Side Effects
Photosensitivity reactions are clinically significant.
Patients should:
- Use broad-spectrum sunscreen
- Avoid excessive sun exposure
- Wear protective clothing outdoors
Neurological Symptoms
Some patients experience:
- Fatigue
- Dizziness
- Reduced energy levels
Weight Loss
Weight reduction may occur in some patients receiving long-term therapy.
Liver Toxicity and Monitoring
Liver monitoring is one of the most important safety considerations during Pirfenidone therapy.
Why Liver Monitoring Is Necessary
Pirfenidone may elevate hepatic enzymes, particularly during treatment initiation or dose escalation.
Recommended Laboratory Monitoring
Pulmonologists commonly monitor:
- ALT
- AST
- Bilirubin
- Alkaline phosphatase
Monitoring Schedule
Before Starting Treatment
Baseline liver function testing.
During First Six Months
Regular monthly monitoring is commonly recommended.
Long-Term Maintenance
Periodic monitoring based on clinical judgment.
Warning Signs Requiring Immediate Medical Attention
Patients should seek urgent medical evaluation if they develop:
- Yellowing of skin or eyes
- Dark urine
- Severe fatigue
- Persistent nausea
- Right upper abdominal pain
Drug Interactions
Because Pirfenidone is metabolized by CYP1A2, several clinically important interactions may occur.
Potentially Significant Drug Interactions
Fluvoxamine
May significantly increase Pirfenidone exposure.
Ciprofloxacin
May alter drug metabolism.
Smoking
Smoking induces CYP1A2 activity and may reduce treatment effectiveness.
Herbal Supplements
Some supplements may influence hepatic metabolism.
Patients should always provide a complete medication list to healthcare providers.
Pirfenidone vs Nintedanib
Nintedanib is another antifibrotic medication widely used in IPF management.
Comparative Overview
| Feature | Pirfenidone | Nintedanib |
|---|---|---|
| Drug Class | Antifibrotic | Tyrosine kinase inhibitor |
| Common GI Effect | Nausea | Diarrhea |
| Photosensitivity | More common | Less common |
| Liver Monitoring | Required | Required |
| Dosing Schedule | Multiple daily doses | Twice daily |
Treatment Selection Considerations
Choice of therapy depends on:
- Patient tolerance
- Pulmonary specialist recommendation
- Liver function status
- Gastrointestinal sensitivity
- Insurance access
- Comorbid conditions
Long-Term Safety Considerations
Long-term antifibrotic therapy requires continuous evaluation of:
- Liver safety
- Weight changes
- Nutritional status
- Adherence patterns
- Pulmonary function trends
Adherence Challenges
Patients may struggle with:
- Complex dosing schedules
- Persistent nausea
- Sun sensitivity precautions
- Chronic disease fatigue
Early patient education significantly improves treatment adherence.
Patient Counseling and Lifestyle Recommendations
Patients receiving Pirfenidone should be educated about:
Smoking Cessation
Smoking may reduce therapeutic effectiveness.
Sun Protection
Strict sun protection reduces photosensitivity risk.
Nutritional Support
Taking medication with food may improve tolerability.
Routine Follow-Up
Regular pulmonary and laboratory monitoring remains essential.
Who Should Avoid Pirfenidone?
Pirfenidone may not be appropriate for:
- Severe hepatic impairment
- Severe renal dysfunction
- Patients with serious hypersensitivity reactions
- Individuals unable to tolerate antifibrotic therapy
Treatment decisions should always be individualized by qualified healthcare professionals.
Expert Medical Perspective
From a pulmonary medicine standpoint, Pirfenidone remains one of the most clinically important disease-modifying therapies available for idiopathic pulmonary fibrosis.
Although it does not reverse established fibrosis, substantial evidence supports its role in slowing pulmonary decline and preserving functional stability.
Optimal outcomes depend on:
- Early diagnosis
- Appropriate patient selection
- Liver monitoring
- Adherence support
- Specialist supervision
Frequently Asked Questions
Is Pirfenidone a cure for IPF?
No. Pirfenidone does not cure pulmonary fibrosis but may slow disease progression.
Can Pirfenidone improve breathing?
Some patients experience stabilization of symptoms and slower lung function decline.
Why is liver monitoring important?
Pirfenidone may elevate liver enzymes, making routine monitoring essential.
Can smokers take Pirfenidone?
Smoking may reduce medication effectiveness and is strongly discouraged.
How long do patients take Pirfenidone?
Treatment duration varies depending on disease progression, tolerability, and physician recommendations.
Internal Linking Recommendations
To strengthen topical authority and avoid orphan-page signals, internally link this article to:
- Pirfenidone dosage guide
- Pirfenidone side effects
- Pulmonary fibrosis symptoms
- Interstitial lung disease overview
- Nintedanib vs Pirfenidone
- https://984online.com/antifibrotic-drugs/Antifibrotic therapy guide
- Liver monitoring during antifibrotic treatment
- IPF survival and prognosis guide
Structured Data Recommendations
Implement the following schema markup:
- MedicalWebPage Schema
- FAQ Schema
- Physician Reviewed Schema
- Article Schema
- Breadcrumb Schema
- Organization Schema
Conclusion
Pirfenidone remains a cornerstone antifibrotic therapy for idiopathic pulmonary fibrosis and related progressive fibrotic lung diseases.
Compared with low-quality AI-generated pharmaceutical summaries, high-E-E-A-T medical content should provide:
- Evidence-based clinical analysis
- Pharmacological depth
- Proper safety guidance
- Scientific citations
- Expert-reviewed medical information
When properly optimized with strong semantic structure, internal linking, medical references, and expert review signals, this type of article can compete more effectively in Google’s YMYL medical search ecosystem.
Medical Disclaimer
This article is intended for educational and informational purposes only and does not replace professional medical advice, diagnosis, or treatment. Patients should consult a pulmonologist, pharmacist, or qualified healthcare provider before starting or modifying Pirfenidone therapy.
